Alzheimer’s Disease: Pathophysiology and Nutritional Implications Rand T. Akasheh Ancestral Health Society – Ancestral Health Symposium University of Illinois at Chicago
Alzheimer disease (AD) is a degenerative disease of cerebral cortex.
Its principal clinical manifestation is dementia and progressive loss of cognitive function, especially memory and learning.
AD is the most common form of dementia in the elderly; AD affects approximately 5 million people in the US. The prevalence is similar in men and women.
Regardless of etiology, dementia is not part of normal aging and always represents a pathologic process.
Patients rarely become symptomatic before age 50.
The incidence of AD increases with age, starting from 1% at 60-64 years and reaching 40%or more at 85-89 years.
AD may be either sporadic or familial.
Most cases of AD cases (95%) are sporadic, while approximately 5% of the cases are familial.
Sporadic AD occurs at older age (late onset, senile), while familial AD occurs earlier in mid life (early onset).
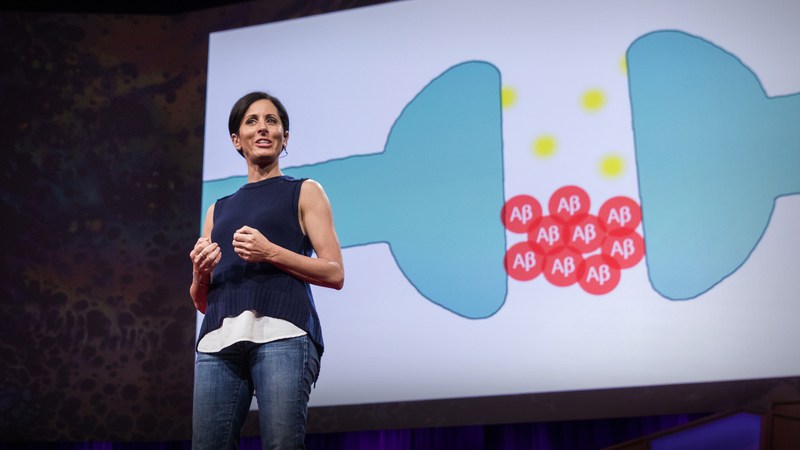
Alzheimer disease is characterized by the presence of plaques and tangles.
Plagues are made by Amyloid-B, aptide derived from a large molecule called amyloid precursor protein (APP).
Plaques are present between cells, in the intercellular space.
Tangles are made by the protein tau. Tangles are intracellular, present in the cytoplasm.
ALZHEIMER’S DISEASE AND DIABETES
GLUCOSE HYPOMETABOLISM IN ALZHEIMER’S DISEASE
INSULIN AND ALZHEIMER’S DISEASE
CAN KETONE REPLACE GLUCOSE IN ALZHEIMER’S DISEASE?
KETONE BODIES AND NEUROLOGICAL DISEASES
ENERGY RESTRICTION AND ALZHEIMER’S DISEASE
CLINICAL IMPLICATIONS FOR DIABETES-RELATED ALZHEIMER’S DISEASE